What is helpful and what isn’t
Helpful
- Compliance with medication.
- Maintaining hydration. Unless instructed otherwise,1.5 litres of water in addition to your usual diet is a great start
- Avoid Kidney Toxins. Usually unkowningly prescribed by doctors. Phone us if in doubt. Avoid fads, specious dietary advice, nostrums and excessive naturopathy. Young enthusiastically voluble pharmacists, naturopaths, concerned friends and neighbours are not the best sources of advice. Kidney Medicine is tough medicine; seek counsel carefully.

1. BLOOD PRESSURE CONTROL
- There is an abundance of evidence, that tight blood pressure control, particularly in the presence of proteinuria, slows the progression of renal disease.
- There is evidence, that the use of ACE inhibitors or Angiotensin Receptor Blocking drugs in diabetics with kidney disease affords particular benefit to slowing the progression towards renal failure.
2. ATHEROGENIC CHOLESTEROL (LDL)
- Reduction of dyslipidaemia does not contribute to slowing the progression of renal disease.
- It will however, reduce the relative risk of heart attack and stroke by up to 20%.
- Most patients will benefit from tight lipid control.
- Remember, the consequences of renal disease is accelerated cardiovascular disease.
3. DIABETIC CONTROL AND THE PROGRESSION OF DIABETIC KIDNEY DISEASE
- Diabetic control which may lead to hypoglycaemia is no longer recommended.
- Diabetic control, particularly if implemented early with metformin, reduces the risk of microvascular disease such as diabetic kidney disease.
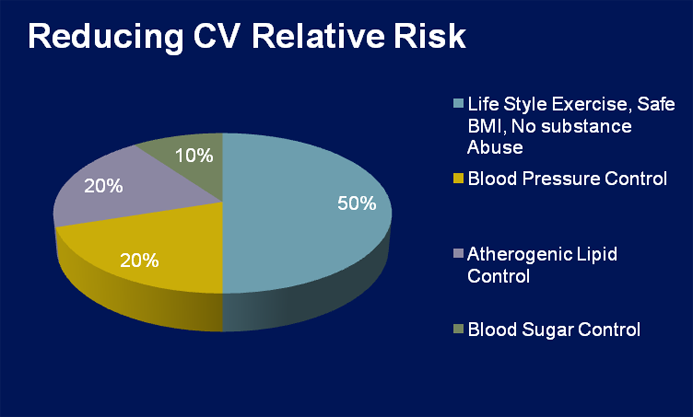
4. EXERCISE
- Control of blood pressure, atherogenic lipids and sugar contribute up to 50% to the reduction of relative risk of cardiovascular disease
- The remaining 50% benefit is contributed by moderate exercise
5. CALCIUM
- Maintaining a normal serum calcium is important, as both reduced calcium, excessive calcium, reduced phosphate or excessive phosphate have been associated with increased mortality.
- Generally calcium is maintained without calcium supplementation, to avoid the possibility of calcium deposition in blood vessels and heart.
- Calcium levels are maintained in association with the treatment of secondary hyperparathyroidism with Calcitriol. This treatment reduces the development of Rena bone disease
6. ACIDOSIS
- There is little evidence acidosis treatment retards the progression of kidney disease.
- However when acidosis is significant, modest treatment with alkali therapy may be beneficial in reducing metabolic bone disease, provided the alkali treatment does not contribute to excess salt intake.
7. PREGNANCY
- Pregnancy should be approached with great caution, when the creatinine clearance is < 60ml/minute (Stage III chronic kidney disease), particularly if the patient has poorly controlled hypertension.
- Pregnancy in renal disease should be planned with the advice of the Nephrologist for the close and careful management of metabolic issues and hypertension from conception to delivery.
Unhelpful
1. PROTEIN RESTRICTION – GENERALLY NOT RECOMMENDED
- Some patient’s report symptomatic relief in Stage IV and V chronic kidney disease.
- Protein restriction < 0.8g/kg may contribute to body fabric decay that occurs in chronic disease, and this is counterproductive.
- Modest protein restriction is sometimes useful in selective conditions, such as kidney stone disease.
2. URIC ACID
- There is little evidence lowering uric acid retards renal failure progression.
- Reduction of uric acid with Allopurinol is indicated in patients suffering gout or impending gout.
3. PHOSPHATE
- Restricting phosphate prior to dialysis is not recommended as it is not practical . It seems to retard renal failure progression in rats but not found to be useful in patients.
Summary
Appropriate treatment of blood pressure, lipids, sugar, a healthy robust diet and moderate exercise with a good lifestyle (no smoking and moderate alcohol), would seem to be the means to retard the progression of renal failure and reduce the risk of death from cardiovascular disease. (i.e. the usual consequence of renal failure).